9.0 Pacific Blue Cross Claim Statements
9.1 Overview
Pacific Blue Cross will issue a statement to the Provider outlining Claim payment details. If you have registered for PROVIDERnet you can access your Claim statements through your account. If you do not have PROVIDERnet you will receive paper Claim statements.
Understanding Your Statement
The details of the statements are outlined below:
Header Information
| 1. Provider Name and Address | This is your mailing address. |
| 2. Date | The date the statement was produced. |
| 3. Your ID Number | Your Pacific Blue Cross Provider ID. |
| 4. Page Number | Current page of the statement. |
| 5. Cheque number/direct deposit Number | The payment number that appears on a physical cheque attached to the statement or on the Electronic Funds Transfer (EFT) statement. |
Health Claim Summary
| 6. Total Amount Claimed | The total amount of each of the Claims for all Members on the statement. |
| 7. Amount Paid by PBC Plan | The total amount covered by the Policy. |
| 8. Total Payment Amount | The total payment amount once any Co-payments and Deductible have been satisfied. |
Claim Details
| Field | Description |
|---|---|
| 9. Claim ID | The number assigned to each transaction. |
| 10. Service Date | The date shown is the exact date the Equipment or Services were purchased. |
| 11. Qty | The quantity. |
| 12. Product or Service | The description of the Equipment or Services. |
| 13. Claimed Amount | The total cost of the Equipment or Services. |
| 14. Eligible Amount | The amount that is an Eligible Expense. |
| 15. Deductible Amount | The amount applied to the Deductible under the Policy (if applicable). |
| 16. Co-payment Amount | The portion the Member pays out of pocket. |
| 17. Percent Covered | The percentage of the total cost of the Equipment or Services that is covered under the Policy. |
| 18. Plan Paid Amount | The amount paid under the Policy. |
| 19. Message Code | The explanation of Claim payment or reason for refusal. |
| 20. Policy Number | This identifies the Policy. |
| 21. ID Number | This identifies each Member. |
| 22. Patient Name | The name of the primary individual eligible under the Policy, or their dependents. |
9.2 Sample Statement
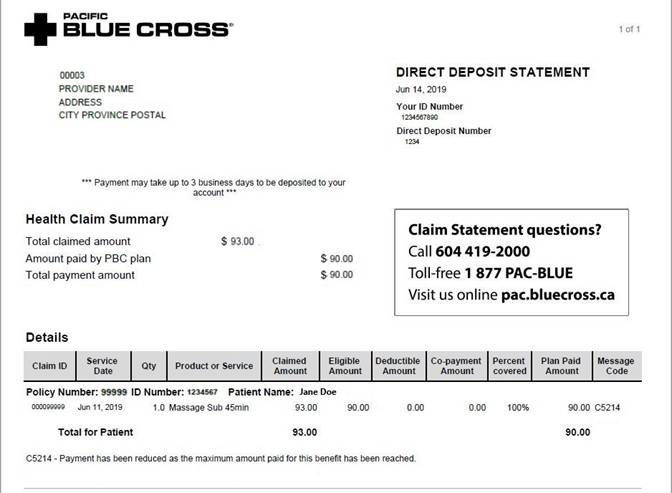
Claim Statement questions?
Call 604 419-2000
Toll-free 1 877 PAC-BLUE
Visit us online pac.bluecross.ca
Toll-free 1 877 PAC-BLUE
Visit us online pac.bluecross.ca